Our Community
Pip’s Story
 When Pip was a puppy, he sadly had to have one of his back legs amputated.
When Pip was a puppy, he sadly had to have one of his back legs amputated.
Pip’s carer recently noticed that he had been struggling to walk for long periods of time on his remaining back leg, and so he was referred to The Ralph for his lameness to be assessed.
Our Orthopaedic team examined Pip’s left hip and noticed he was experiencing a lot of discomfort on extension of the leg and that he also had a severely reduced range of motion (the extent to which a body part can be moved around a joint) of the hip joint.
X-rays confirmed the presence of severe arthritis in the ball and socket of the hip joint.
In a normal hip joint, the ball (femoral head) fits securely into a deep, smooth and rounded socket (acetabulum). Cartilage protects the bones from rubbing against each other and getting damaged.
If the joint develops abnormally, it becomes unstable and loose, which means the ball no longer fits into the socket correctly. Over time, the friction causes arthritis, resulting in pain, discomfort and lameness.
Together with Pip’s carers, the team discussed treatment options for Pip – either a total hip replacement, or a femoral head ostectomy (“floating joint” surgery) – and it was decided that a total hip replacement would be the best option to support Pip’s weight.
What was involved in Pip’s total hip replacement?
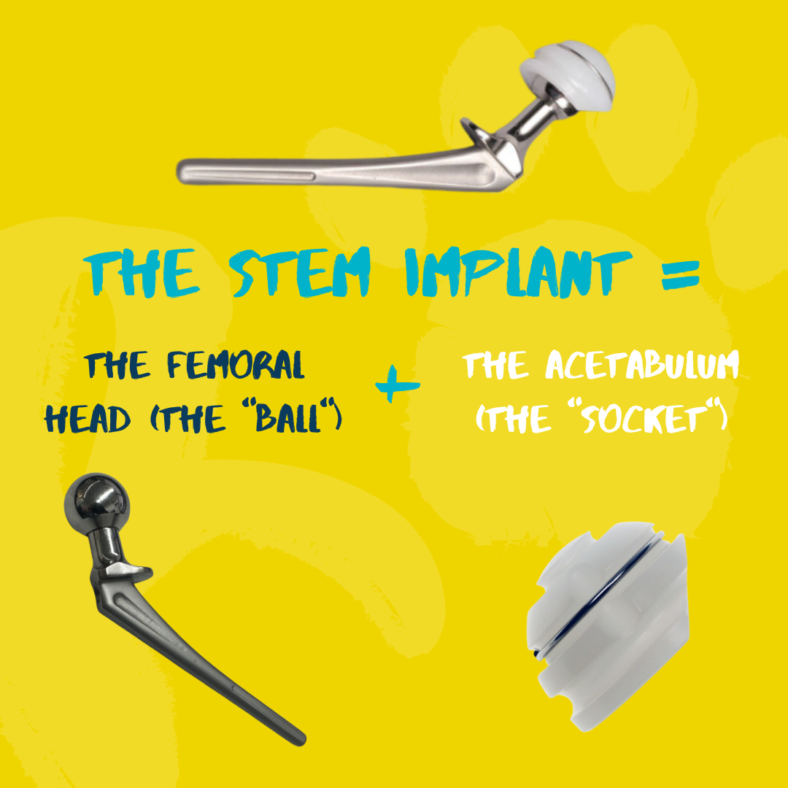
The orthopaedic surgeon removes the femoral head (the “ball”) completely using a surgical saw. The acetabulum (the “socket”) is then made by an artificial cup shape that can be cemented or press-fit into place.
A stem implant is then inserted through the centre of the pre-prepared femur bone (thigh bone). The surgeon then attaches a femoral head (“ball”) implant to the top of the femur bone.
The “ball and socket” components are then placed together again and the reconstruction of the hip joint is complete.
In Pip’s case, an iliofemoral suture was also placed. This synthetic suture was placed to avoid excessive outer rotation of the limb whilst all of Pip’s weight was held on that limb and reduce he risk of dislocation.
Post-operative X-rays confirmed good positioning of the implant, and Pip recovered well from the surgery.
He returned for a check up a few months later and Pip was comfortable walking, but on examination our team found that Pip’s hip region was more swollen than expected. Manipulation of Pip’s left hip failed to show smooth movement of the head within the socket, suggesting that the hip had luxated (dislocated). The risk of luxation was much higher in this case due to Pip only having three legs. This suspicion was confirmed by an X-ray.
The following day, Pip underwent correction surgery. The artificial cup implant which was placed during the previous surgery – a cementless cup – was completely integrated, and needed to be removed with a high-speed surgical bur (a tool to cut bone). The team replaced the previous cup with a cemented cup.
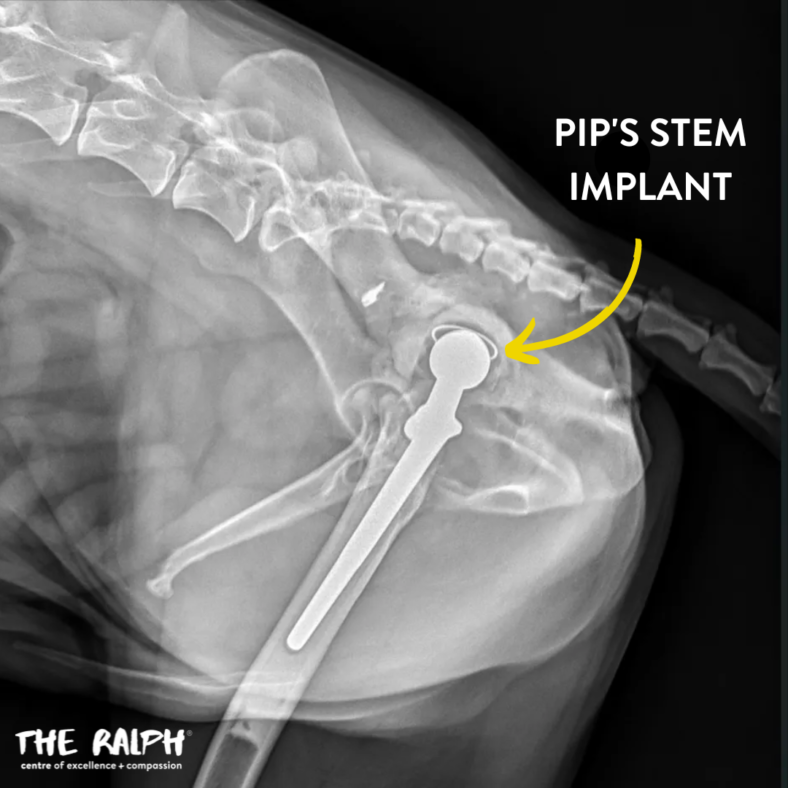
Post-operative X-rays again confirmed satisfactory implant position, and Pip recovered smoothly from the procedure and was discharged home to continue his recovery at home.
Six weeks later, Pip came back to us for a check-up to see how he was getting on. Pip’s carers reported that he appeared to be walking comfortably on his back leg.
X-rays confirmed the implant was still in good position, and a physical examination found that Pip now has normal range of motion in the hip joint with no restrictions.
A total hip replacement is a true team effort, from the surgeons, anaesthetists, theatre and anaesthesia nurses, wards nurses, patient care assistants and the patient’s family. Every person is vital before, during and after surgery to ensure the smoothest outcome for the patient.